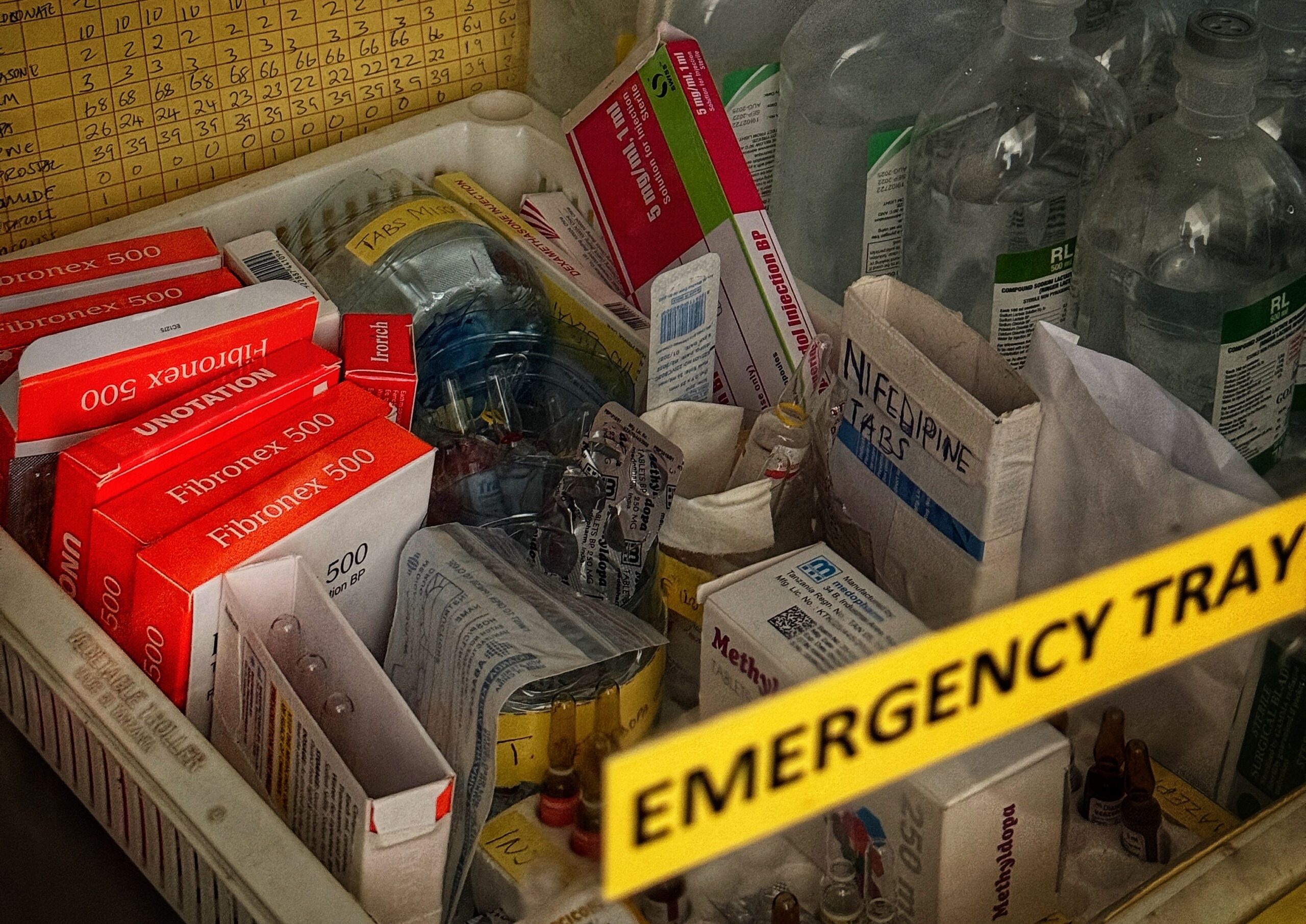
Three ways that TXA can cut severe bleeding and save blood stocks





Sign up for the WOMAN Trials newsletter for all the latest news and exclusive updates on the WOMAN Trials and to join our global movement working towards safe childbirth for women everywhere, regardless of income, location or background.