We can look at maternal deaths when demanding better maternal healthcare for women.
Frame the story where it resonates – would you accept a commuter van full of people crashing every day? That is the reality: a van full of women is dying every single day.”
– Dorah Kiconco Musinguzi, Raising Voices, community advisor
Preventing maternal deaths starts with listening to the communities affected. In 2023, just over 90% of all maternal deaths occurred in lower-middle-income countries according to the World Health Organization. Postpartum haemorrhage (PPH) is what most maternal deaths are attributed to worldwide.
Tranexamic acid (TXA), an effective treatment that reduces severe bleeding after birth, has been shown to save lives when given quickly. Yet access remains limited in many settings, particularly where women give birth outside of hospitals or where trained staff are not immediately available.
The I’M WOMAN Trial is investigating whether TXA can be given as an intramuscular injection, making it faster and easier to deliver in obstetric emergencies. But understanding how this treatment could reach women in time, if proven effective, depends on more than research alone.
Alongside our research, our Community Advisory Board (CAB) brings together maternal health advocates, clinicians, legal experts and community leaders from across Nigeria, Kenya, Tanzania, Ethiopia and Pakistan. Their role is to ensure the current evidence on TXA for PPH treatment reflects the realities of the communities it aims to serve.
The following perspectives from the CAB, also known as community advisors, will help the I’M WOMAN Trial understand ways to improve maternal health and support equitable access to TXA.
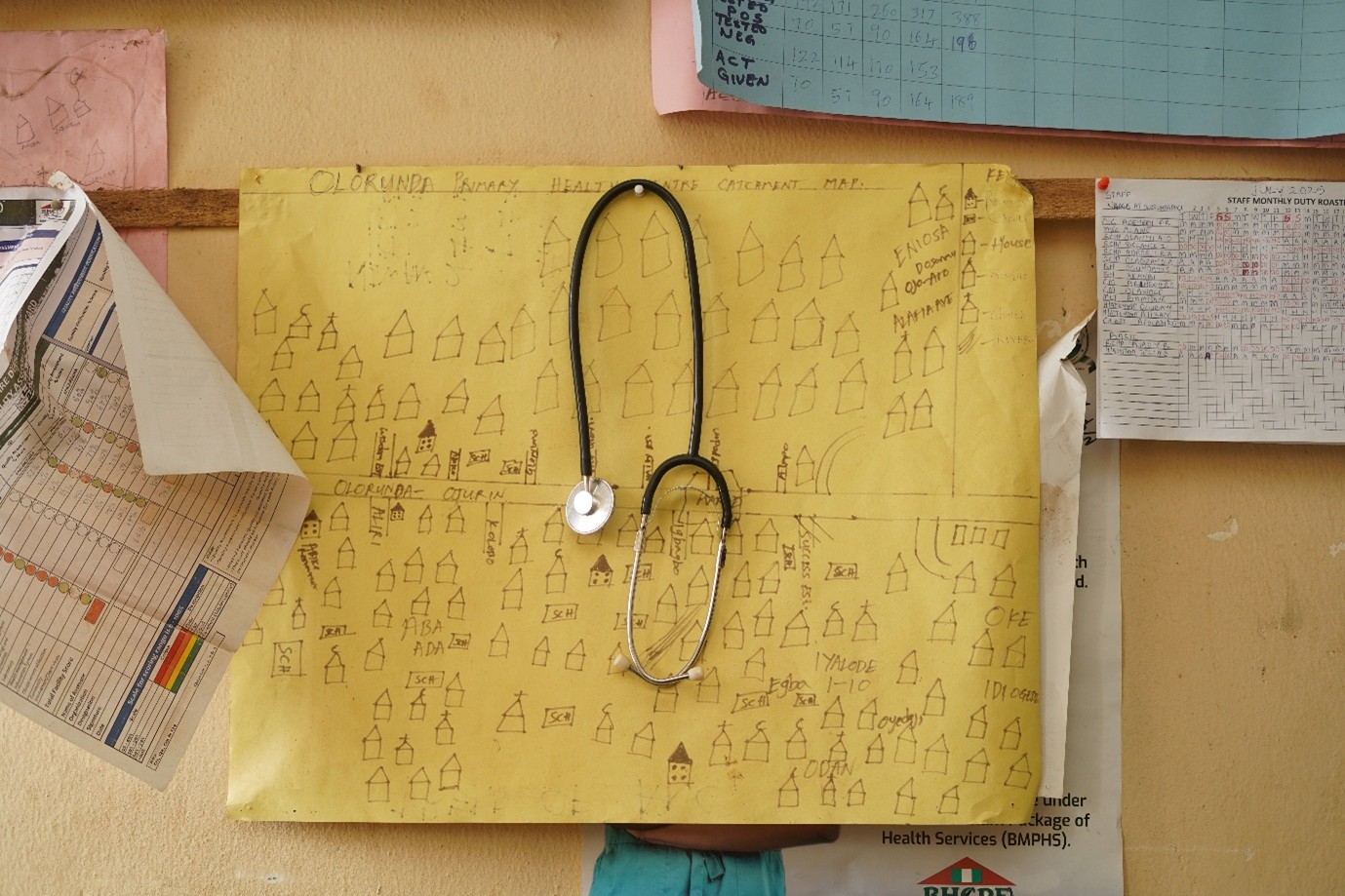
The CAB includes Women Advocates Research and Documentation Centre (WARDC) who are working with the I’M WOMAN Trial’s TRANSFORM project by speaking to communities in Nigeria to raise awareness of PPH.